
Incident Investigation Improved by Applying the Event Causation Technique: A Case Study
By Sufiana Safiena1 and Goh Yang Miang2 | 15th Apr 2020
1Research Assistant, Safety and Resilience Research Unit (SaRRU), Department of Building, School of Design and Environment, National University of Singapore. E-mail: bdgssak@nus.edu.sg
2Associate Professor, Safety and Resilience Research Unit (SaRRU), Department of Building, School of Design and Environment, National University of Singapore. E-mail: bdggym@nus.edu.sg
1 Introduction
A company involved in port operations contacted the Safety and Resilience Research Unit (SaRRU) to review their incident investigation of a near-miss during discharge of cargo. The company was unable to identify the root cause of the incident. The company sent their investigation report and relevant documents for us to review. We were permitted to share the results of our evaluation. Using the incident as a case study, this article shares some important points for improving the quality of incident investigations.
2 Case Details
Details of the near-miss incident are as follows:
- On 9th September 2019, a group of workers were deployed to discharge steel cargo from a vessel.
- The team used two 12-tonne chain slings (1.5 m each) and two 8-tonne chain slings (9 m each) with Clevis hook to discharge the H-beam steel cargo.
- At 2030hr, one of the 8-tonne lifting gear broke at the link, causing the cargo to drop 1 – 2 feet.
- No injury was reported and work operations were stopped immediately.
- The investigation report stated fatigue of the lifting gear as a contributory factor.
The company also provided the lifting gear (LG) certificate, relevant management system procedures and information, and their investigation report for review. In the LG certificate provided, it shows that the chain slings were purchased in 2016 and were due to expire in 2020. The chain sling that failed was load-tested on 23rd August 2016 and was not yet due for the renewal load proof test. The chain sling passed the visual inspection by an Authorised Examiner (AE) on 30th July 2019, i.e. the LG certificate was valid during the incident.
According to the lifting team, pre-operations checks by the lifting supervisor showed that there was no deformation in the lifting chains prior to the incident and it was able to meet all operational requirements. The AE was engaged to re-inspect the remaining chains in the chain sling that failed. A separate engineering company conducted the visual inspections, load tests, and link measurement on the remaining chains. The remaining chains passed the tests and inspections, and the report by the engineering company being certified by the AE.
Table 1 Incident timeline
| 1800hr | Vessel arrived |
| Manpower consisting of 5 workers, 1 lifting supervisor (LS) and 1 foreman went onboard | |
| 1918hr | Toolbox meeting was conducted before the start of lifting operations |
| 1922hr | Visual inspection of the lifting gears before usage (about 10 mins) |
| 1946hr | Started discharging the H-beam steel cargo from the vessel |
| 2025hr | Incident happened after approximately 7 lifts, the 8-tonne lifting gear broke at the link and the cargo fell 1 – 2 feet |
| There was no injury on site |
3 Areas for Improvement
The areas of improvement for incident investigations are derived based on the Event Causation Technique (ECT)[1](Goh, 2018).
[1] https://worldscientific.com/worldscibooks/10.1142/11094 (2nd edition will be released in 2020/2021)
3.1 Comprehensive Timeline
One way the incident investigation report could have been improved is through the compilation of a comprehensive timeline. A comprehensive timeline is critical for an effective incident investigation because it provides the necessary details to understand the situation that the workers were in. This allows the investigator to assess if the collected facts form a coherent picture. The timeline forms the basis for determination of the root cause or underlying factors and the corresponding recommendations for improvement.
We were able to create a basic timeline (see Table 1) based on the information from the lifting team and a WhatsApp group chat system that the company uses to disseminate operational details.
3.2 Reliability of Evidence
Based on information from the lifting team, the crane operator had indicated that the load could have been stuck, causing excessive tension on the lifting gear leading to its failure. Even though this was not considered plausible by the company, the reason for eliminating this possible direct cause should be discussed in the investigation report.
It is noted that the company requested the same AE who inspected the LG prior to the incident to re-inspect the LG after the incident. To avoid any potential conflict of interest, it is a good practice to appoint an independent AE to re-inspect the LG after an incident. Nevertheless, the remaining chains in the chain sling that failed (see Figure 1) were inspected and tested by an independent engineering company. However, no failure analysis was conducted to confirm the cause of the failure.

3.3 Evaluation of Safety Measures (Controls)
An investigation team needs to review all controls identified in relevant risk assessments and procedures to determine missing controls, effectiveness of implemented controls, and level of implementation of controls. For example, based on the information collected (see Table 1), the lifting supervisor took about 10 minutes to inspect the lifting chains (2 x 9 m 8-tonne chain sling and 2 x 1.5 m 12.5-tonne chain sling). There was no review of the effectiveness of the visual inspection. An informal inquiry with a lifting engineer showed that 10 minutes to inspect the 4 chain slings may not be sufficient. He recommended 15 – 20 minutes for the inspection. Furthermore, we were unable to confirm if the lighting condition was conducive for visual inspection.
It is unknown how long the toolbox meeting was and if the meeting was effective. An effective toolbox meeting should be based on relevant risk assessment and should allow workers to participate in the discussion. The supervisor should also ask some questions to check that information disseminated during the toolbox meeting was understood by the workers.
3.4 Determination of the Root Cause
The main reason the company approached us is because they were unable to determine the root cause of the incident. Based on the incident investigation report, the initial investigation team had labelled “Inspection and Control” as the root cause. Furthermore, a remark, “Lifting gear snapped” was placed next to the root cause. Due to the lack of a failure analysis, the direct cause of the failure was not conclusive. Thus, it is difficult to determine root cause(s).
Assuming that the direct cause is indeed fatigue failure of the chain, then the company must conduct careful evaluation of their operations and maintenance procedures. We realised that the company did not record the number of hours of usage of their lifting gears, and there were no criteria for the retirement of lifting gears. However, there are other possible direct causes such as manufacturer defects and local damage to the chain sling that were not conclusively eliminated.
We prefer using the term “underlying factors” instead of “root cause” because many of these more foundational issues are contributory in nature. In the Event Causation Technique (ECT), underlying factors are made up of 3 main components: management system inadequacies, safety culture and safety leadership. In this investigation, safety culture and leadership were not evaluated. In addition, a more complete evaluation of the management system inadequacies should have been conducted.
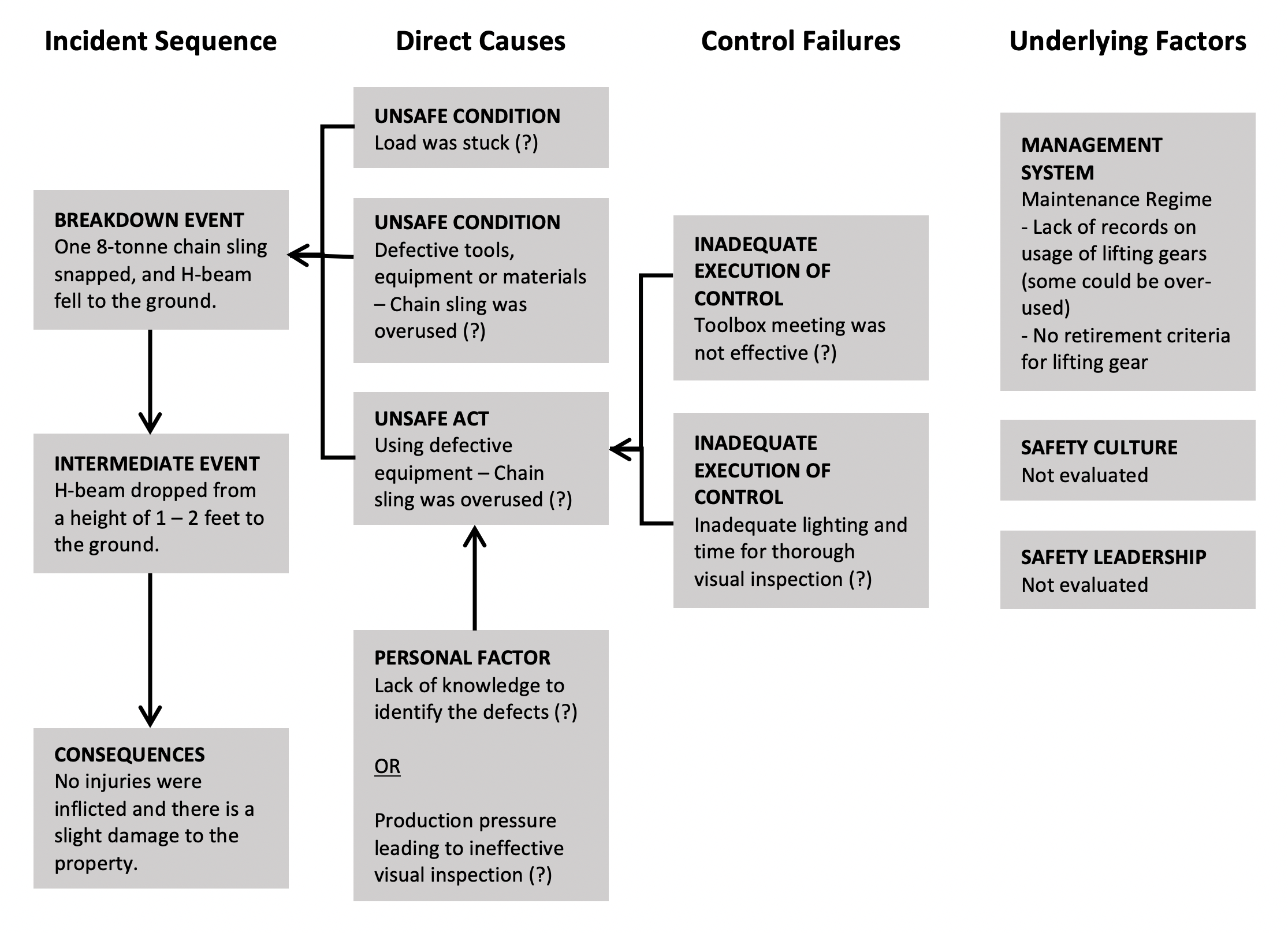
3.5 Systematic Incident Analysis Methods
The ECT framework is a systematic approach to guide investigation and analysis. It is an example of a diagrammatic incident analysis approach that is useful to improve the quality of incident investigation. Figure 2 shows a preliminary ECT diagram that could have been created during investigation to guide the evidence that are required to confirm or eliminate possible direct causes, control failures, and underlying factors. As indicated in Figure 2, there is unconfirmed information that requires further investigation. As highlighted earlier, the underlying factors of safety culture and leadership were not evaluated in the investigation in this case study.
4 Conclusion
Possible Areas for Improvement:
|
Incident investigation is a critical element of any WSH management system. It is important for the investigation to be rigorous and comprehensive to ensure that the organisation can effectively learn from the incident. The areas for improvement identified in this case study can also be observed in many other companies and are not unique to the company involved.
5 References
Goh, Y. M. (2018). Introduction to Workplace Safety and Health Management: World Scientific Publishing Co Pte Ltd.